
The following is a three-part case study illustrating the evaluation, surgical planning, and outcome for a patient with lumbar spondylolisthesis and stenosis who had not improved with prior treatment. All imaging is shared with patient consent for educational purposes.
Part 1: Presentation
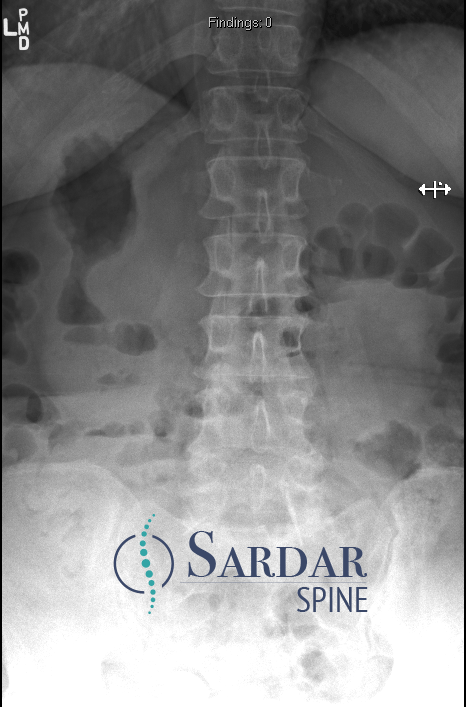
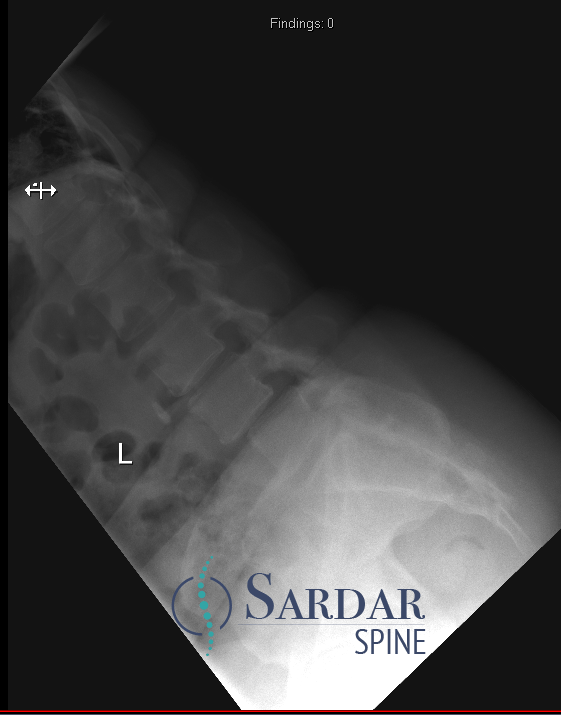
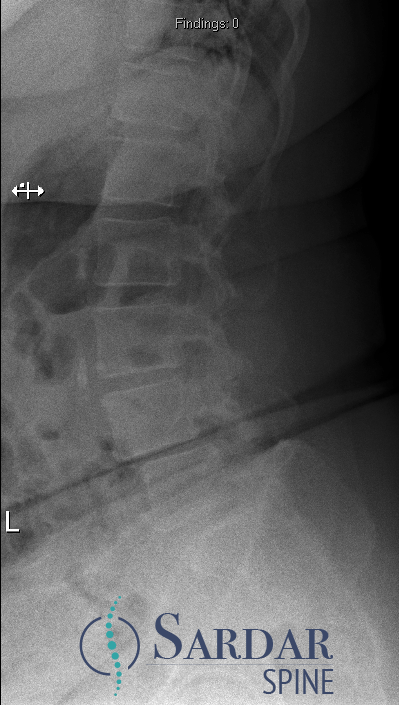
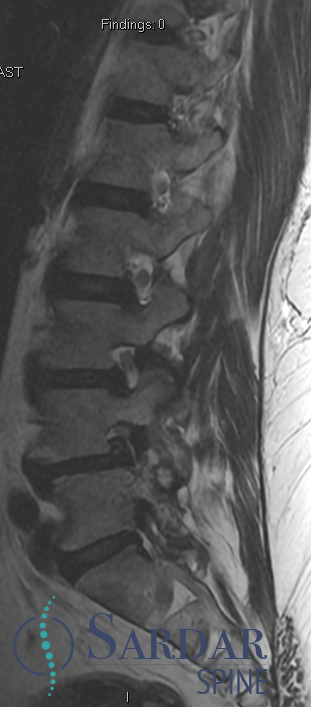
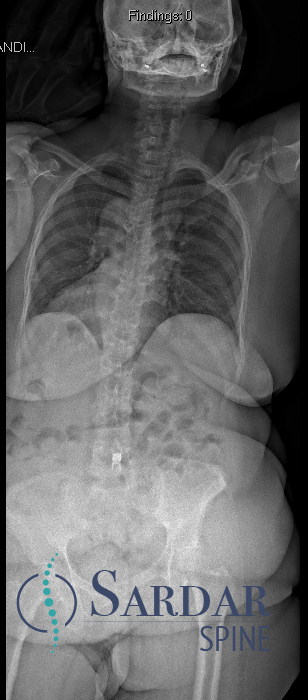
A 55-year-old woman presented with progressive back pain and bilateral leg pain that significantly limited her ability to walk. Imaging confirmed lumbar stenosis and spondylolisthesis at L4-5, disc degeneration at L3-4, and severe arthritis at L5-S1. She had already undergone a course of physical therapy and multiple epidural steroid injections with only short-term relief.
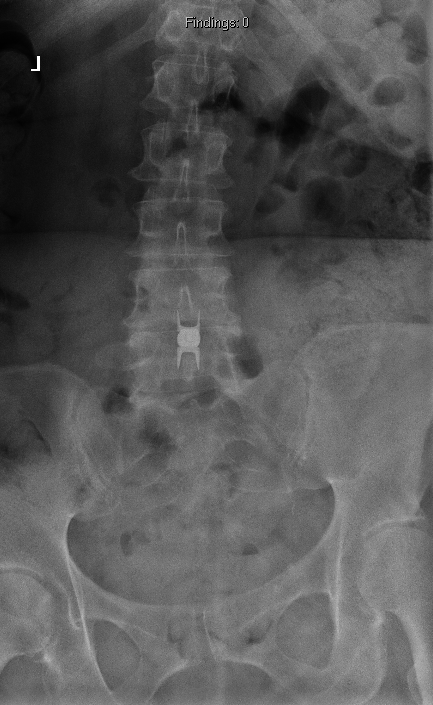
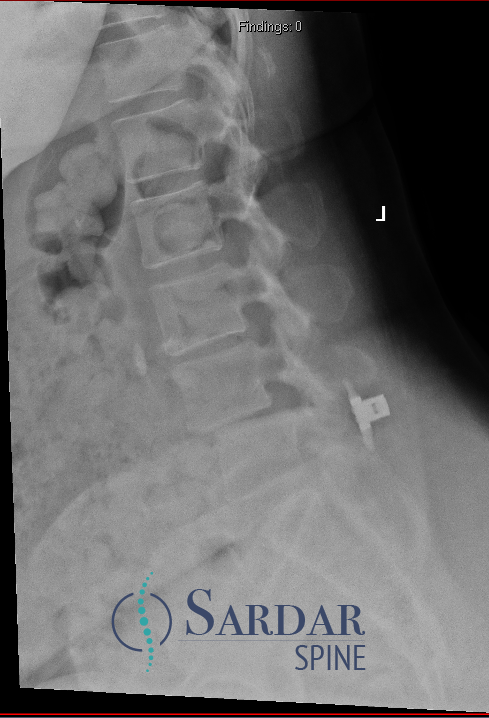
On examination, she had significant difficulty with prolonged standing and walking. Her X-rays on presentation are shown below, demonstrating the degree of listhesis and degenerative change at multiple levels.



Part 2: Failed Prior Treatment and Worsening
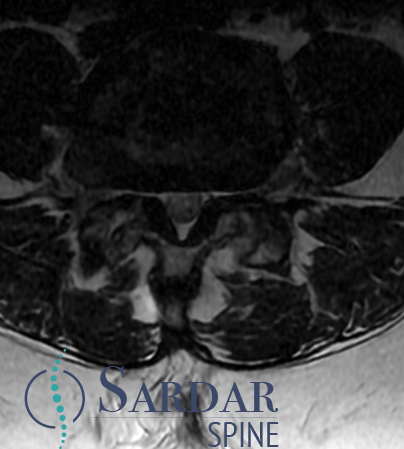
Before presenting to Dr. Sardar, the patient had undergone a Vertiflex interspinous spacer procedure at another institution. Rather than improving her symptoms, the procedure was followed by progressive worsening. By the time of her follow-up evaluation, she was unable to stand upright and required a walker for mobility.
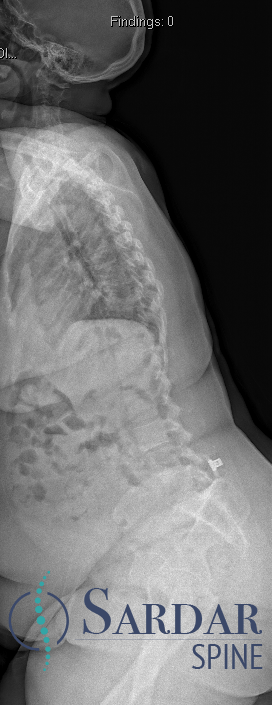
Repeat imaging confirmed that her underlying spondylolisthesis and sagittal malalignment had progressed. The interspinous spacer had not addressed the structural instability at the involved levels, and the added device had not stabilized the segment. Her clinical picture now represented a case of progressive lumbar deformity with neurogenic claudication and functional decline — a pattern that is not amenable to further conservative or minimally invasive intervention.

Part 3: Surgical Treatment and Outcome
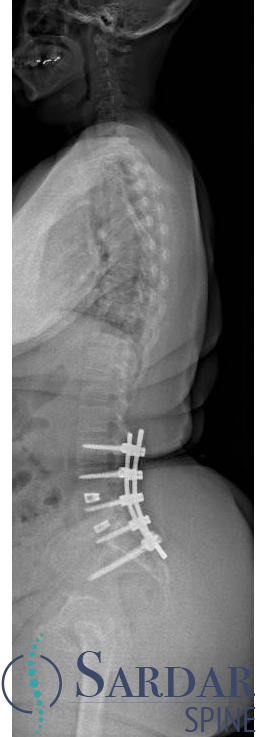
After a comprehensive evaluation — including full-length standing X-rays, CT, MRI, and medical optimization — the patient underwent posterior spinal reconstruction from L3 to S1/ilium with transforaminal lumbar interbody fusion (TLIF) at L4-S1. The Vertiflex device was removed as part of the procedure.
The surgical goals were to decompress the neural elements, restore lumbar lordosis, achieve solid segmental fixation, and correct the overall sagittal alignment. Robotic-assisted navigation was used for pedicle screw placement, and intraoperative neuromonitoring was maintained throughout the case.
At follow-up, the patient was able to stand upright without a walker — a functional milestone she had not achieved in years. Her leg pain resolved and her back pain improved significantly. Post-operative X-rays confirmed solid instrumentation, restored lordosis, and well-balanced sagittal alignment.

Case presented for educational purposes with patient consent. This post does not constitute individualized medical advice. Treatment decisions should be made in consultation with a qualified spine specialist based on individual clinical findings.
About Dr. Zeeshan Sardar
Dr. Sardar is Co-Chief of Spinal Deformity Surgery at NewYork-Presbyterian / Columbia University and specializes in complex spinal reconstruction, revision surgery, and adult spinal deformity. To schedule a consultation, call 212-932-5187 or visit the contact page.
